The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Contenuto fornito da PulmPEEPs. Tutti i contenuti dei podcast, inclusi episodi, grafica e descrizioni dei podcast, vengono caricati e forniti direttamente da PulmPEEPs o dal partner della piattaforma podcast. Se ritieni che qualcuno stia utilizzando la tua opera protetta da copyright senza la tua autorizzazione, puoi seguire la procedura descritta qui https://it.player.fm/legal.
Simile a PulmPEEPs
Five-time winner of Best Education Podcast in the Podcast Awards. Grammar Girl provides short, friendly tips to improve your writing and feed your love of the English language. Whether English is your first language or your second language, these grammar, punctuation, style, and business tips will make you a better and more successful writer. Grammar Girl is a Quick and Dirty Tips podcast.
…
continue reading
Making It is a weekly audio podcast that comes out every Friday hosted by Jimmy Diresta, Bob Clagett and David Picciuto. Three different makers with different backgrounds talking about creativity, design and making things with your bare hands.
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
The Voice of ASWJ Australia. Listen to & Download Our Latest Programs. Topics: Aqeedah (Creed), Tafsir Qur'an, Islamic Fiqh, History, Youth & Community programs, Medical & Health programs and much much more. Podcasts are in Arabic & English.
…
continue reading
Player FM - App Podcast
Vai offline con l'app Player FM !
Vai offline con l'app Player FM !

))
83. RFJC 13 – ARDS Series – DEXA-ARDS
Manage episode 436410782 series 3299598
Contenuto fornito da PulmPEEPs. Tutti i contenuti dei podcast, inclusi episodi, grafica e descrizioni dei podcast, vengono caricati e forniti direttamente da PulmPEEPs o dal partner della piattaforma podcast. Se ritieni che qualcuno stia utilizzando la tua opera protetta da copyright senza la tua autorizzazione, puoi seguire la procedura descritta qui https://it.player.fm/legal.
In the penultimate episode in our ARDS Rapid Fire Journal Club Summer Series we are talking about the DEXA-ARDS trial (published in Lancet Respiratory Medicine in 2020). This trial evaluated the impact of dexamethasone in the treatment of ARDS.
Article and Reference
Today we’re discussing the DEXA-ARDS trial published in Lancet Respiratory Medicine in 2020. This trial evaluated the impact of dexamethasone on mortality and duration of mechanical ventilation for patients with ARDS.
Infographic
Article Notes
- DEXA-ARDS; Lancet Respiratory Medicine, 2020
- DOI:10.1016/S2213-2600(19)30417-5
- Link: https://doi.org/10.1016/s2213-2600(19)30417-5
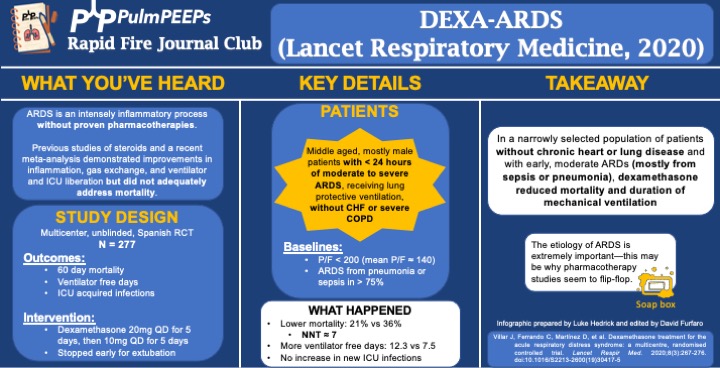
- Background: ARDS is an intense inflammatory process without proven, specific pharmacotherapies. Previous work and a recent meta-analysis demonstrated improvements in inflammation, gas exchange, and ventilator and ICU liberation but did not adequately address mortality.
- Study Design (design, primary outcome, participants, etc)
- Design: investigator-initiated, multicenter, unblinded, randomized controlled trial in 17 academic ICUs in Spain, conducted from 3/2013 to 12/2018
- Primary Outcome
- VFD at 28d
- Secondary:
- 60d mortality
- Actual duration of ventilation in ICU survivors
- ICU acquired infections
- Participants
- Inclusion ARDS with P/F < 200 for < 24hr on LTVV
- Exclusion:
- Already receiving steroids or immunosuppression
- CHF
- Severe COPD
- DNR
- Summary: Middle aged, mostly male patients with < 24hr of moderate to severe ARDS receiving LPV without chronic heart or lung disease
- Like many ARDS trials, just over 3/4 of patients’ ARDS was caused by PNA or sepsis. Mean P/F was ~140
- Intervention/Limitations
- N = 277, stratified by center and then randomized
- Intervention: dexamethasone 20mg qd for 5d followed by 10mg qd for 5d
- Stopped early for extubation before day 10
- First dose given no more than 30 hours after P/F < 200
- Control: no placebo, just SOC
- All patients received LTVV
- Outcomes/Safety
- Power: with N = 314 (actual N = 277), 80% power to detect 2 additional VFD and 15% mortality reduction
- As an aside, this seems to be a theme in ICU trials: massively ambitious proposed benefits during power calculations and then under-enrolling for that power calculation ultimately resulting with a point estimate that favors the intervention but is not statistically significant.
- Efficacy:
- 60d mortality: 21% vs 36%, P = 0.0047
- NNT of just < 7!
- VFD at 28d: 12.3 vs 7.5, P < 0.0001
- Actual duration of ventilation in ICU survivors: 14.2d vs 19.5d (P = 0.0009)
- 60d mortality: 21% vs 36%, P = 0.0047
- Safety:
- Hyperglycemia: 76% vs 70%, P = 0.33
- Always interesting in steroid trials when no change in glucose control is seen. This isn’t the most EBM thing I’ll ever say, but frankly I disregard this and assume steroids will cause hyperglycemia regardless of the trial results.
- ICU acquired infections: 24% vs 25%, P = 0.75
- Hyperglycemia: 76% vs 70%, P = 0.33
- Power: with N = 314 (actual N = 277), 80% power to detect 2 additional VFD and 15% mortality reduction
- Takeaway
- In a narrowly selected population of patients without chronic heart or severe lung disease and with early, moderate ARDS (mostly from sepsis or pneumonia), dexamethasone reduced mortality and duration of mechanical ventilation.
- If time, insert soap-box about etiology of ARDS being very important (EG, flu, fungal, parasitic, mycobacterial infections)
- In a narrowly selected population of patients without chronic heart or severe lung disease and with early, moderate ARDS (mostly from sepsis or pneumonia), dexamethasone reduced mortality and duration of mechanical ventilation.
85 episodi
Manage episode 436410782 series 3299598
Contenuto fornito da PulmPEEPs. Tutti i contenuti dei podcast, inclusi episodi, grafica e descrizioni dei podcast, vengono caricati e forniti direttamente da PulmPEEPs o dal partner della piattaforma podcast. Se ritieni che qualcuno stia utilizzando la tua opera protetta da copyright senza la tua autorizzazione, puoi seguire la procedura descritta qui https://it.player.fm/legal.
In the penultimate episode in our ARDS Rapid Fire Journal Club Summer Series we are talking about the DEXA-ARDS trial (published in Lancet Respiratory Medicine in 2020). This trial evaluated the impact of dexamethasone in the treatment of ARDS.
Article and Reference
Today we’re discussing the DEXA-ARDS trial published in Lancet Respiratory Medicine in 2020. This trial evaluated the impact of dexamethasone on mortality and duration of mechanical ventilation for patients with ARDS.
Infographic
Article Notes
- DEXA-ARDS; Lancet Respiratory Medicine, 2020
- DOI:10.1016/S2213-2600(19)30417-5
- Link: https://doi.org/10.1016/s2213-2600(19)30417-5
- Background: ARDS is an intense inflammatory process without proven, specific pharmacotherapies. Previous work and a recent meta-analysis demonstrated improvements in inflammation, gas exchange, and ventilator and ICU liberation but did not adequately address mortality.
- Study Design (design, primary outcome, participants, etc)
- Design: investigator-initiated, multicenter, unblinded, randomized controlled trial in 17 academic ICUs in Spain, conducted from 3/2013 to 12/2018
- Primary Outcome
- VFD at 28d
- Secondary:
- 60d mortality
- Actual duration of ventilation in ICU survivors
- ICU acquired infections
- Participants
- Inclusion ARDS with P/F < 200 for < 24hr on LTVV
- Exclusion:
- Already receiving steroids or immunosuppression
- CHF
- Severe COPD
- DNR
- Summary: Middle aged, mostly male patients with < 24hr of moderate to severe ARDS receiving LPV without chronic heart or lung disease
- Like many ARDS trials, just over 3/4 of patients’ ARDS was caused by PNA or sepsis. Mean P/F was ~140
- Intervention/Limitations
- N = 277, stratified by center and then randomized
- Intervention: dexamethasone 20mg qd for 5d followed by 10mg qd for 5d
- Stopped early for extubation before day 10
- First dose given no more than 30 hours after P/F < 200
- Control: no placebo, just SOC
- All patients received LTVV
- Outcomes/Safety
- Power: with N = 314 (actual N = 277), 80% power to detect 2 additional VFD and 15% mortality reduction
- As an aside, this seems to be a theme in ICU trials: massively ambitious proposed benefits during power calculations and then under-enrolling for that power calculation ultimately resulting with a point estimate that favors the intervention but is not statistically significant.
- Efficacy:
- 60d mortality: 21% vs 36%, P = 0.0047
- NNT of just < 7!
- VFD at 28d: 12.3 vs 7.5, P < 0.0001
- Actual duration of ventilation in ICU survivors: 14.2d vs 19.5d (P = 0.0009)
- 60d mortality: 21% vs 36%, P = 0.0047
- Safety:
- Hyperglycemia: 76% vs 70%, P = 0.33
- Always interesting in steroid trials when no change in glucose control is seen. This isn’t the most EBM thing I’ll ever say, but frankly I disregard this and assume steroids will cause hyperglycemia regardless of the trial results.
- ICU acquired infections: 24% vs 25%, P = 0.75
- Hyperglycemia: 76% vs 70%, P = 0.33
- Power: with N = 314 (actual N = 277), 80% power to detect 2 additional VFD and 15% mortality reduction
- Takeaway
- In a narrowly selected population of patients without chronic heart or severe lung disease and with early, moderate ARDS (mostly from sepsis or pneumonia), dexamethasone reduced mortality and duration of mechanical ventilation.
- If time, insert soap-box about etiology of ARDS being very important (EG, flu, fungal, parasitic, mycobacterial infections)
- In a narrowly selected population of patients without chronic heart or severe lung disease and with early, moderate ARDS (mostly from sepsis or pneumonia), dexamethasone reduced mortality and duration of mechanical ventilation.
85 episodi
Tutti gli episodi
×Benvenuto su Player FM!
Player FM ricerca sul web podcast di alta qualità che tu possa goderti adesso. È la migliore app di podcast e funziona su Android, iPhone e web. Registrati per sincronizzare le iscrizioni su tutti i tuoi dispositivi.
Simile a PulmPEEPs
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Five-time winner of Best Education Podcast in the Podcast Awards. Grammar Girl provides short, friendly tips to improve your writing and feed your love of the English language. Whether English is your first language or your second language, these grammar, punctuation, style, and business tips will make you a better and more successful writer. Grammar Girl is a Quick and Dirty Tips podcast.
…
continue reading
Making It is a weekly audio podcast that comes out every Friday hosted by Jimmy Diresta, Bob Clagett and David Picciuto. Three different makers with different backgrounds talking about creativity, design and making things with your bare hands.
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
The Voice of ASWJ Australia. Listen to & Download Our Latest Programs. Topics: Aqeedah (Creed), Tafsir Qur'an, Islamic Fiqh, History, Youth & Community programs, Medical & Health programs and much much more. Podcasts are in Arabic & English.
…
continue reading
Player FM - App Podcast
Vai offline con l'app Player FM !
Vai offline con l'app Player FM !



